
The Benefits of Universal Healthcare
Lower costs and so much more!

Universal Healthcare has been a popular idea in the US for over a decade. I remember reading during the 2016 election cycle that over half of the country supported universal healthcare. As of late 2025, it is up to 64% (Daniller, 2025). While not as high as its peak in 2006, support for universal healthcare has been steadily rising for the past decade (Daniller, 2025). “Universal healthcare” can mean different things to different people. It could mean guaranteed health insurance for all Americans, or it could be a single-payer system like the UK, Canada, or Taiwan. For the rest of this article, I will be using “universal healthcare” to mean a single-payer system like Medicare-for-All.
What is universal healthcare/Medicare-for-All?
Universal healthcare/Medicare-For-All is “a single-payer, government-run health care program in which all Americans are covered and which replaces almost all other existing public and private plans” (Sarlin & Kimelman, 2019). Single-payer is when “a single public or quasi-public agency takes responsibility for financing healthcare for all residents” (Sylvie, 2016). In other words, government pays the hospital bill instead of the patient. While each country implements it a little differently, the above remains the same. Most of the hospitals in the UK are government owned. The proposed single payer model in the US would keep hospitals private, but they would bill the government instead of the patient and/or the patient’s insurance. No more copays, no more worrying about whether treatment is covered by insurance, no more fighting with insurance companies to get them to pay what their policy claims they’ll pay. Best of all, no more medical debt! Easy and cheap!
But just because universal healthcare is easy and cheap doesn’t mean it’s good. What are the benefits of universal healthcare and why is it better than our current system?
Lower Costs
Universal Healthcare is cheaper. Between 2023 and 2033, Americans are projected to spend $42.9T ($55T in 2025 dollars) on healthcare (Federal Reserve Bank of Minneapolis, 2026; Public Citizen, 2025). That includes both private a federal spending. According to Public Citizen (2025), “Medicare for All spending would be approximately $37.8 trillion between 2017 and 2026.” Converting that to 2025 dollars, that’s $49.6T (Federal Reserve Bank of Minneapolis, 2026). Still less than what we’re projected to spend on the current system.
Why the decrease? Private expenditures mostly disappear with universal healthcare. People no longer have to worry about the copays, insurance premiums, and/or out-of-network expenses they currently pay. Most American families will save thousands of dollars a year. A family making $75,000/year could save over $9000 (Flannery, 2026)! That would be like getting a 12% raise! This is consistent with another study stating universal healthcare “likely to lead to a 13% savings in national healthcare expenditure” (Galvani et al., 2021).
The right-wing, Koch-funded Mercatus Center stated in 2018 that single-payer healthcare would cost us $32.6T between 2022 and 2031(Balhous, 2018). That’s around $42T in 2025 dollars (Federal Reserve Bank of Minneapolis, 2026). So even the most conservative (pun intended) estimates show universal healthcare saving us money!
But what about taxes?
One of the main criticisms of universal healthcare is it will increase our taxes. Some economists argue it would cut taxes for most Americans, but for the sake of discussion let’s assume it will raise them (Saez & Zucman, 2019). Senator Bernie Sanders has stated multiple times universal healthcare will increase our taxes (Thomas & Regan, 2016). Indeed, his proposed bill does contain a tax increase, but an increase in taxes doesn’t mean Americans will pay more. According to National Nurses United (2024), “even with the tax increase proposed by legislators, 95% of Americans will pay less than they do now. The taxes would replace premiums, co-pays, and deductibles.” So even with higher taxes, universal healthcare will be cheaper for almost all Americans than the current model.
Increased Bargaining Power
Over 65% of Americans are dependent on private health insurance to cover the costs of care (Keisler-Starkey & Bunch, 2024). That insurance is usually provided through employers, which reduces the cost of the insurance for the employees. While this may sound like a good deal for employees, it’s actually a good deal for employers. Employers get tax breaks for providing their employees with insurance and it gives them an important bargaining chip against unions (Delaney, 2020; Desmond, 2023).
Even with Obamacare, most people can’t afford the quality of health insurance they receive without their employers. Corporations know this and use health insurance when negotiating with unions. This makes it harder for unions to secure better pay, improved working conditions, and better benefits for their employees. Universal healthcare would shift power away from corporations (Delaney, 2020).
With universal healthcare, employees would no longer depend on their employers for health insurance. Employees will have more leverage at the negotiating table both as individuals and as unions. It also improves the economy by allowing for greater employee mobility. This brings me to another problem caused by our existing healthcare system: job lock.
Universal Healthcare Reduces Job Lock
Job lock is when people choose to stay in a job because they’re afraid of losing their health insurance. While it other benefits can also cause job lock, it’s usually health insurance.
When employers know their employees won’t relocate due to health insurance, it allows them to make cuts in other areas. Employees receive lower pay and worse working conditions. It also leads to lower earning potential because the employee is stuck at a job that refuses to give them raise when they could be moving to new jobs that offer better pay and/or better fit their skills.
According to Teirlinck & Stoilova (n.d.), job lock hurts the overall economy by lowering productivity and stifling innovation. It’s exactly what I learned in business school. Labor mobility to essential for increasing economic growth (raising GDP). People need to be able to go where they’re needed so they can find positions that better use their skills and increase their earning potential. People being unable to change jobs stifles economic growth. Slower economic growth contributes to a lower quality of life for a country.
Reduced Poverty
The cost of medical treatment and the impact of medical debt on US households have been topics of discussion for decades. Even people who don’t support universal healthcare understand how expensive healthcare is. Despite having insurance, most Americans have had to pay hundreds—or even thousands—of dollars for a medical expense (myself included). According to GoFundMe’s CEO, a third ($650M) of all the website’s payouts go to healthcare costs (Martinez, 2023). Even with that, 40% of Americans still have some form of medical debt (Sparks et al., 2026). That debt has pushed some of them into poverty. Universal healthcare would reduce poverty by preventing further medical debt. In my opinion, any universal healthcare bill should come with medical debt forgiveness.
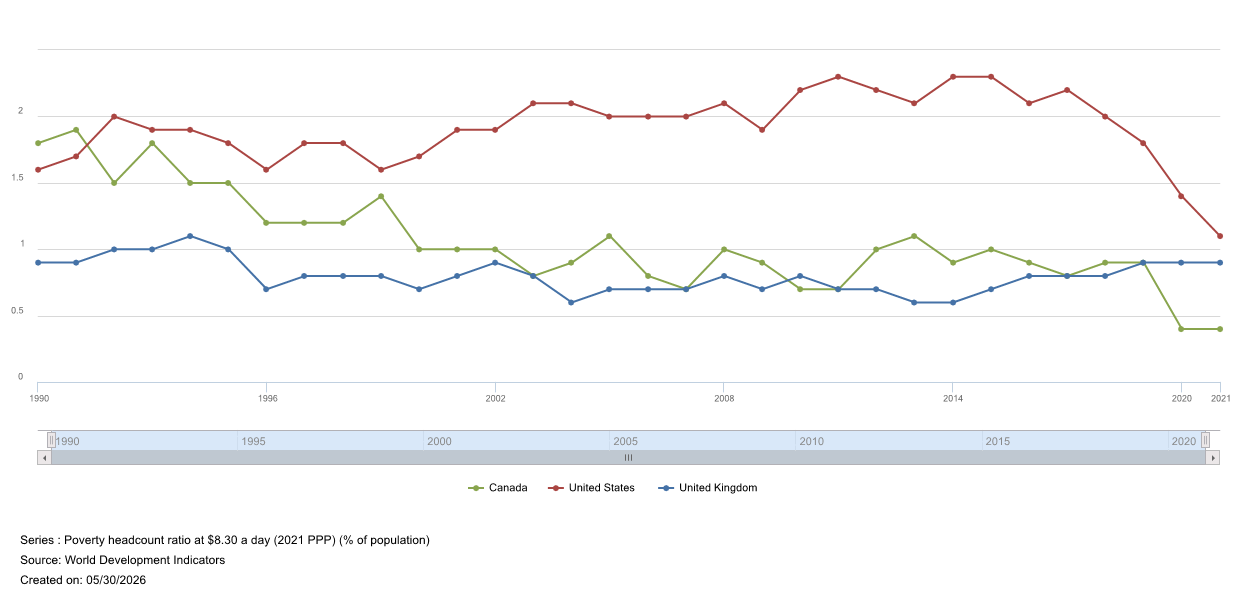
While the cost of medical debt is a problem, another issue not frequently discussed is how sickness impacts income. Sick people earn less money and are less able to gain and maintain employment. It’s not because they’re “lazy” or “weak,” it’s because many of them don’t have sufficient access to the medicine and/or treatment they need. Worse, if people go without treatment long enough, manageable conditions can turn into more serious ones. For example, Type II Diabetes can lead to kidney failure or limb amputations if it goes untreated (Desmond, 2023). Universal healthcare allows people with certain health conditions to gain the treatment they need and remain healthy enough to maintain employment. Access to medical treatment is one of the reasons why poverty rates in countries with universal healthcare like the Canada and the UK are lower than they are here in the US.
Before I move on, I want to go on record saying I don’t think people who are sick—or anyone, really—should be forced to work. I don’t believe one of the advantages of universal healthcare is being able to push people with chronic conditions into the workforce “because now they can afford treatment.” This is one of the many reasons why I support Universal Basic Income. The only reason I’m discussing this at all is because there are many people who want to work but can’t because their inability to get treatment for their medical conditions prevents them from doing so. Finally, I would be remiss if I didn’t mention the biggest obstacle people with medical conditions face is employment discrimination (Harris et al., 2019). No amount of medicine is going to cure bigotry. We need to do better as a society on that front!
Better Quality of Care
Most importantly, universal healthcare improves the quality of care. The Centers for Medicare and Medicare (2025) define quality of outcome as “the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge.” A healthcare outcome “is defined as the results or consequences of treatment or healthcare” (Klose, 2016). Putting these two together, the quality of care is measured by positive health outcomes.
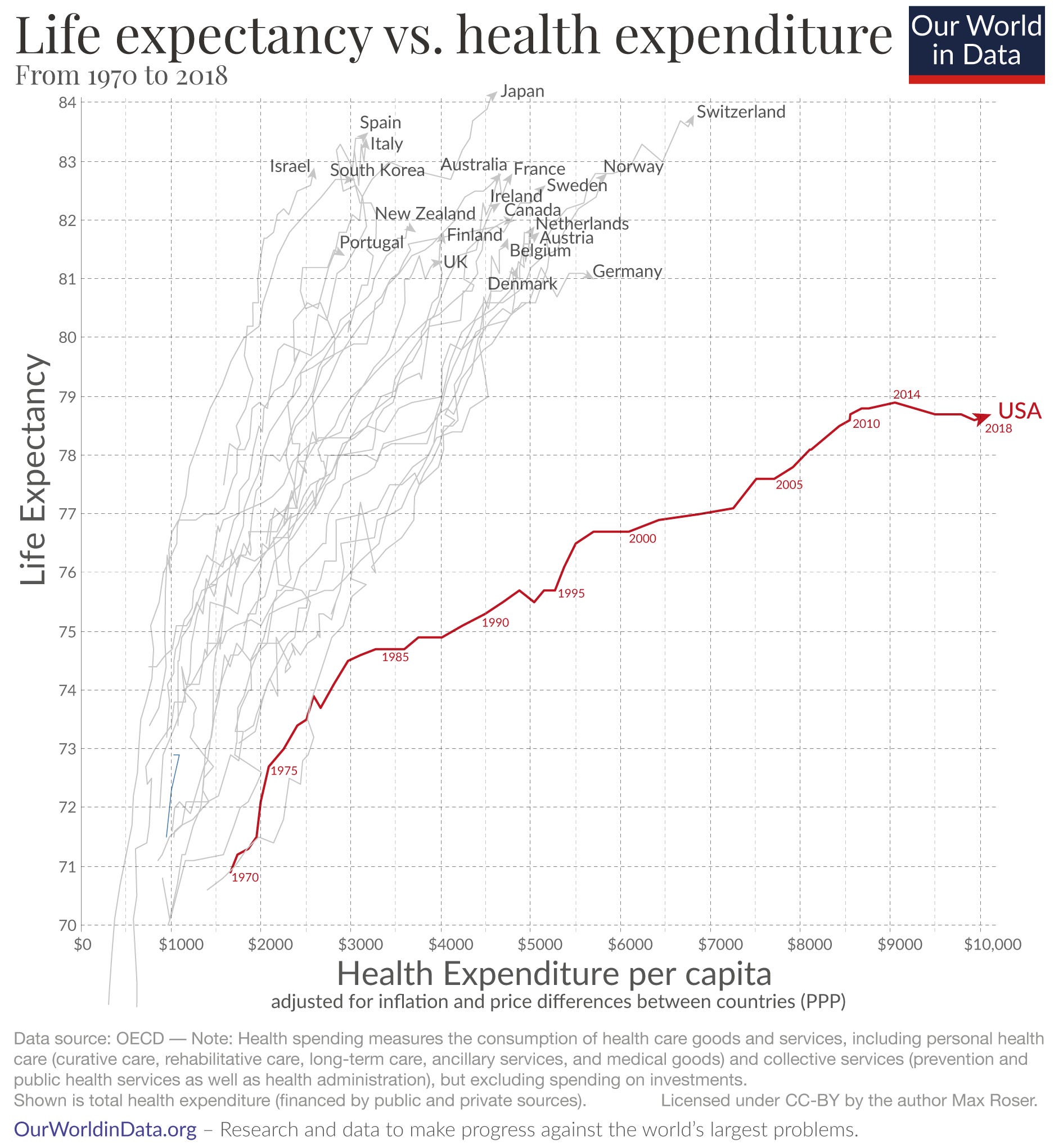
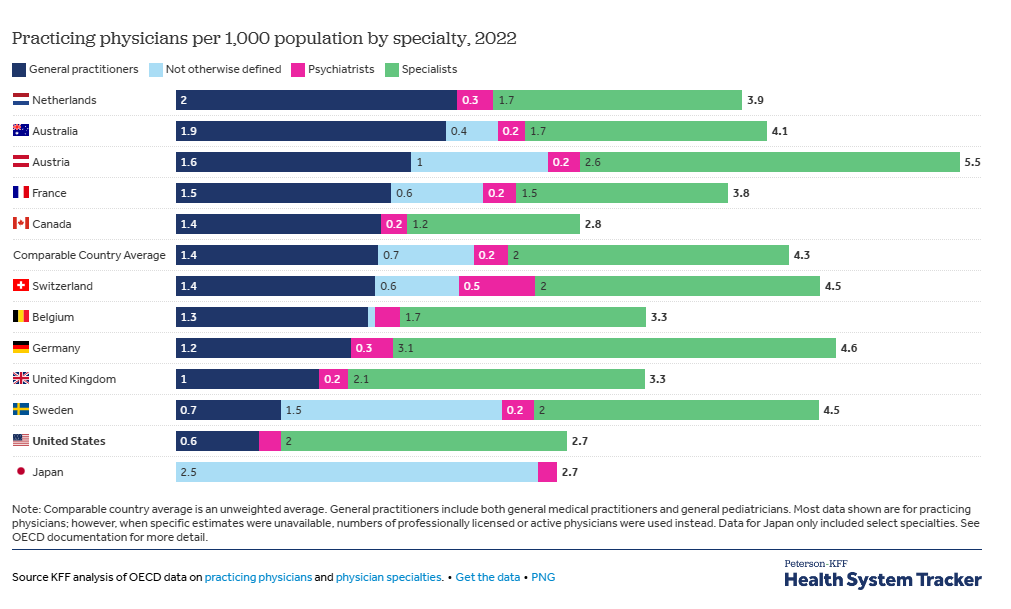
The US is the only developed country without universal healthcare and has the worst care. Compared to ten other countries, including Canada and the UK, the US ranked last in overall healthcare and specifically in access to care and healthcare outcomes (Blumental et al., 2024). Most notably, our life expectancy is lower than those of the other countries and this is despite spending more on healthcare than they do (see above chart). Our infant mortality rate is also the highest in the developed world and is especially bad for Black children (Jang & Lee, 2022; Petrullo, 2023).
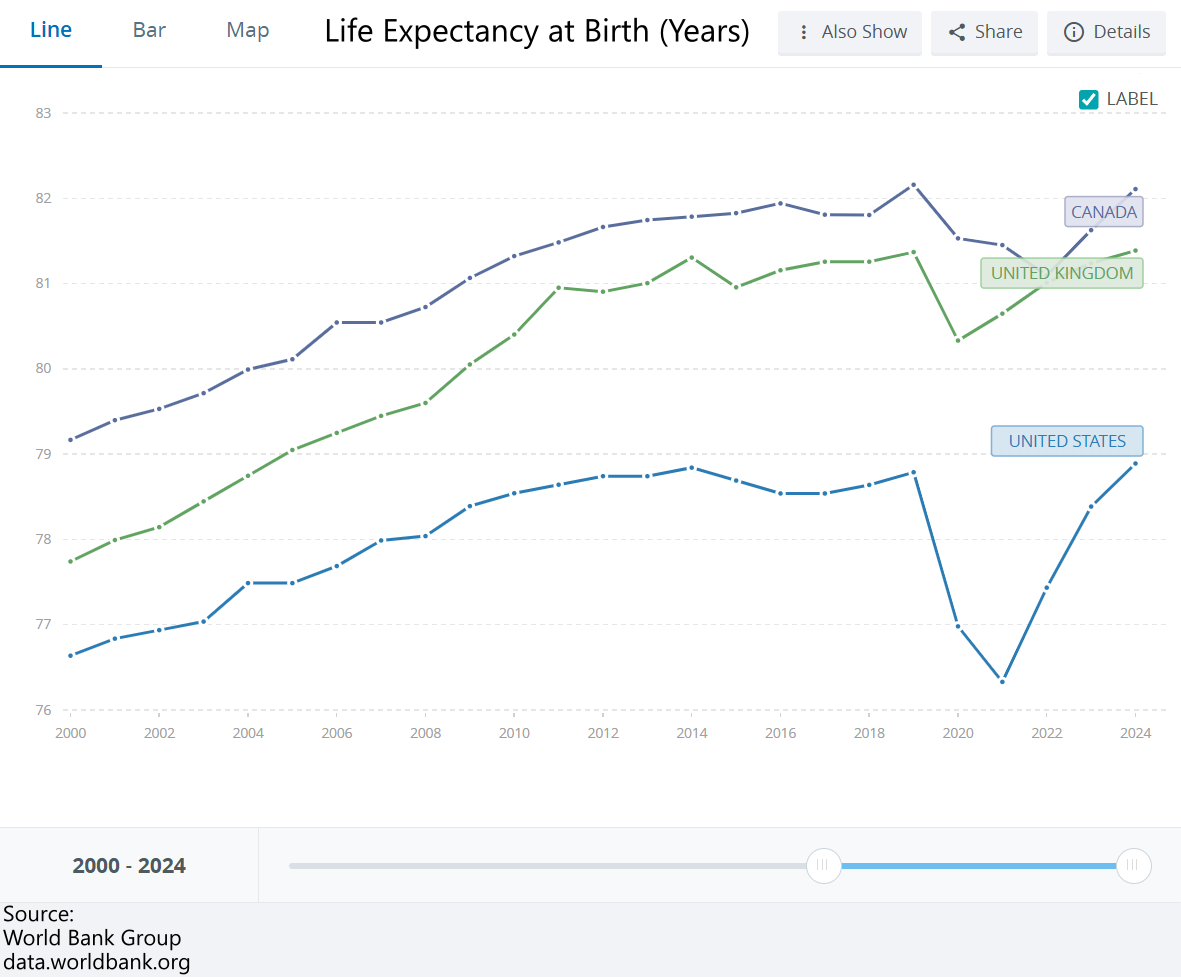
Not having universal healthcare significantly hindered our ability to response to COVID-19. “If the U.S. had had a single-payer universal health care system in 2020, nearly 212,000 American lives would have been saved that year, according to a new study” (Blair, 2022). It also would’ve been cheaper. With universal healthcare, “the country would have saved $105 billion in COVID-19 hospitalization expenses alone” (Blair, 2022). Even worse, the US saw a larger dip in life expectancy because of the pandemic vs. the UK and Canada (World Bank Group, 2026).
Additionally, the US has fewer doctors per 1000 people than many other developed nations (Telesford et al., 2025). This shortage of doctors has hit rural areas in the US extra hard because populations are smaller and people are poorer (Horstman et al., 2025; Kettles, 2025). Fewer hospitals can afford to operate in these areas, leading to monopolies. Even metropolitan areas face increased healthcare costs due to monopolization (AHIP, 2026). On top of this, many US doctors are moving to countries like Canada. While Trump was the reason many doctors were fleeing north in 2025, this has been a problem since before Trump won in 2016 (Glauser, 2014; Kelman, 2025). Another reason they’re moving north is Canada pays their doctors better than America does. “Increased pay is the main driver of this interest. Philpott said family physicians, pediatricians and psychiatrists can make $100000 more annually in Canada, on average, compared to the US” (Glauser, 2014). With private healthcare, profits determine how much a medical facility can pay their physicians. A public system creates opportunities for them to be paid more since profit is no longer the goal. This contradicts the claim made by critics that universal healthcare will lead to doctor shortages in the US. If the other countries are an indicator, universal healthcare will increase the number of doctors available in the US!
One problem not discussed often is how healthcare costs and medical debt make our health worse. This is mainly due to people delaying treatment because it’s too expensive. Even people with insurance have this problem:
Many insured adults said they or a family member had delayed or skipped needed health care or prescription drugs because they couldn’t afford it in the past 12 months: 29 percent of those with employer coverage, 37 percent covered by marketplace or individual-market plans, 39 percent enrolled in Medicaid, and 42 percent with Medicare (Collins et al., 2023).
As mentioned in the previous section, not being able to afford treatment can make health problems worse. And as health problems get worse, they get more expensive to treat. Buying medications for Type II Diabetes is less expensive than dialysis for kidney failure due to diabetic nephropathy. Medicare-4-All would remove the costs associated with healthcare and allow people to get diagnosed with and treated for diseases while they’re easier and less expensive to manage. To quote Tay Zonday, “Poverty charges interest.”
But what about “wait times?”
Critics of universal healthcare love to bring up “wait times” as a reason to not to implement it. There are multiple different problems with this criticism, but I’m only going to focus on three.
First, “wait times” is a weasel phrase. It has different meanings depending on who you ask, but it’s treated as if it has only one. This is also known as an equivocation fallacy. What specific wait times are critics discussing? Wait times for elective surgery? Wait times to see their primary care physicians or other forms of preventative medicine? Wait times for to see a specialist? Wait times for emergency room visits? It could mean waiting for any number of different parts of the medical system, some of which people may care about less than others. So when people talk about wait times, they need to specify which wait time they’re discussing. Then they need to provide evidence supporting that wait time and why that wait time means the US shouldn’t adopt universal healthcare.
Second, there’s one wait time critics never discuss: the wait times of people who can’t afford medical treatment. Regardless of what “wait time” is being discussed, their wait is infinite! While the Affordable Care Act (Obamacare) has reduced this number of people, there are still millions of Americans per year who go without treatment because they can’t afford the costs of medical treatment (USAFacts Team, 2026). Over 68,000 of those Americans will die (Office of U.S. Sen. Bernie Sanders, 2023).
Finally, depending on which wait times we’re discussing, they could be shorter under universal healthcare! Under Medicare only 21% of seniors wait more than 4 weeks to see a specialist (National Nurses United, 2020). Many European countries have shorter wait times to see a primary care physician/general practitioner. “According to a recent study by the Consumer Choice Center, the average wait for a GP appointment in the United States in 2023 was around three weeks, two to ten times longer than in Europe” (Fleck & Richter, 2024).
Down with Private Healthcare!
In conclusion, our current healthcare system is garbage. Not only is it more expensive than universal healthcare, but it provides worse service too. Critics of universal healthcare like to mock the Canadian system, but our doctors are lining up to work there! While Canada’s system is far from perfect, it still provides more benefits at lower costs than our system. They live longer than we do, for example. Additionally, they don’t have to worry about losing their healthcare when their boss lays them off to do stock buybacks. America faces multiple problems due to economic inequality. In addition to improving people’s health, universal healthcare would be a great first step in combatting them!
Sources:
AHIP. (2026, March 30). Rise of hospital monopolies causing ‘elevated concerns’ of ‘increased…. AHIP. https://www.ahip.org/news/articles/rise-of-hospital-monopolies-causing-elevated-concerns-of-increased-prices-less-access-to-care-worries-about-patient-safety-quality
Balhous, C. (2018, July 30). The costs of a national single-payer healthcare system. Mercatus Center. https://www.mercatus.org/research/working-papers/costs-national-single-payer-healthcare-system
Blair, J. (2022, June 20). Study: More than 335,000 lives could have been saved during pandemic if U.S. had Universal Health Care. Yale School of Public Health. https://ysph.yale.edu/news-article/yale-study-more-than-335000-lives-could-have-been-saved-during-pandemic-if-us-had-universal-health-care/
Blumenthal, D., Gumas, E. D., Shah, A., Gunja, M. Z., & Williams, R. D. (2024, September 19). Health care by country 2024 report | commonwealth fund. The Commonwealth Fund. https://www.commonwealthfund.org/publications/fund-reports/2024/sep/mirror-mirror-2024
Centers for Medicare & Medicaid Services. (2025, February 27). Quality of Care. CMS.gov. https://www.cms.gov/priorities/innovation/key-concepts/quality-care
Collins, S. R., Roy, S., & Masitha, R. (2023, October 26). Paying for it: How health care costs and medical debt are making Americans sicker and poorer. The Commonwealth Fund. https://www.commonwealthfund.org/publications/surveys/2023/oct/paying-for-it-costs-debt-americans-sicker-poorer-2023-affordability-survey
Daniller, A. (2025, December 10). Is ensuring health care coverage a government responsibility? what Americans think. Pew Research Center. https://www.pewresearch.org/short-reads/2025/12/10/most-americans-say-government-has-a-responsibility-to-ensure-health-care-coverage/
Delaney, J. (2020, February 14). Medicare for all helps unions by taking health care off the bargaining table [truthout]. Health Care For Us. https://hc4us.org/medicare-for-all-helps-unions-by-taking-health-care-off-the-bargaining-table-truthout/
Desmond, M. (2023). Poverty, by America. Crown.
Federal Reserve Bank of Minneapolis. (2026). Inflation Calculator. Federal Reserve Bank of Minneapolis. https://www.minneapolisfed.org/about-us/monetary-policy/inflation-calculator
Flannery, M. E. (2026, May 12). The education case for single-payer healthcare systems. NEA. https://www.nea.org/nea-today/all-news-articles/education-case-single-payer-healthcare-systems
Fleck, A., & Richter, F. (2024, September 17). Infographic: Healthcare: How long do patients have to wait?. Statista Daily Data. https://www.statista.com/chart/33079/average-waiting-times-for-a-doctors-appointment/?srsltid=AfmBOooFprQl5SyrASayXsUC2n9_AwzaQWrhDw_4b2LDV4iazjqUijBX
Galvani, A. P., Parpia, A. S., Foster, E. M., Singer, B. H., & Fitzpatrick, M. C. (2020). Improving the prognosis of health care in the USA. The Lancet, 395(10223), 524–533. https://doi.org/10.1016/s0140-6736(19)33019-3
Glauser, W. (2014). US doctors migrating north. Canadian Medical Association Journal, 186(11). https://doi.org/10.1503/cmaj.109-4805
Harris, S. P., Gould, R., & Mullin, C. (2019). Research brief: Experience of discrimination and the ada. Research Brief: Experience of Discrimination and the ADA | ADA National Network. https://adata.org/research_brief/experience-discrimination-and-ada
Horstman, C., & Shah, A. (2025, November 17). The state of Rural Primary Care in the United States. The Commonwealth Fund. https://www.commonwealthfund.org/publications/issue-briefs/2025/nov/state-rural-primary-care-united-states
Jang, C., & Lee, H. (2022). A review of racial disparities in infant mortality in the US. Children, 9(2), 257. https://doi.org/10.3390/children9020257
Keisler-Starkey, K., & Bunch, L. N. (2024, September 11). Health insurance coverage in the United States: 2023. Census.gov. https://www.census.gov/library/publications/2024/demo/p60-284.html
Kelman, B. (2025, May 29). American doctors look to relocate to Canada to avoid the Trump administration. NPR. https://www.npr.org/sections/shots-health-news/2025/05/29/nx-s1-5414345/american-doctors-look-to-relocate-to-canada-to-avoid-the-trump-administration
Kettles, M. (2025, May 16). Op-ed: Market failures and the cost of Rural Health Inequality. Michigan Journal of Economics. https://sites.lsa.umich.edu/mje/2025/05/16/op-ed-market-failures-and-the-cost-of-rural-health-inequality/
Klose, K., Kreimeier, S., Tangermann, U., Aumann, I., & Damm, K. (2016). Patient- and person-reports on healthcare: Preferences, outcomes, experiences, and satisfaction – an essay. Health Economics Review, 6(1). https://doi.org/10.1186/s13561-016-0094-6
Martinez, G. (2023, December 12). GoFundMe CEO: One-third of fundraisers are for medical costs | time. TIME. https://time.com/5516037/gofundme-medical-bills-one-third-ceo/
National Nurses United. (2020, January 25). Frequently Asked Questions. Medicare For All. https://medicare4all.org/about/#1579909967320-c582ff39-dcc8
National Nurses United. (2024, September 9). Flyers. Medicare For All. https://medicare4all.org/flyers-2/
Office of U.S. Sen. Bernie Sanders. (2023). Fact Sheet Medicare for All 2023. Martin Heinrich. https://www.heinrich.senate.gov/download/fact-sheet-medicare-for-all-2023
Petrullo, J. (2023, January 31). US Has Highest Infant, Maternal Mortality Rates Despite the Most Health Care Spending. AJMC. https://www.ajmc.com/view/us-has-highest-infant-maternal-mortality-rates-despite-the-most-health-care-spending
Public Citizen. (2025, November 3). Fact check: Medicare for all would save the U.S. trillions; public option would leave millions uninsured, not Garner Savings. Public Citizen. https://www.citizen.org/news/fact-check-medicare-for-all-would-save-the-u-s-trillions-public-option-would-leave-millions-uninsured-not-garner-savings/
Saez, E., & Zucman, G. (2019, October 25). Make no mistake: Medicare for all would cut taxes for most Americans | Emmanuel Saez and Gabriel Zucman. The Guardian. https://www.theguardian.com/commentisfree/2019/oct/25/medicare-for-all-taxes-saez-zucman
Sarlin, B., & Kimelman, J. (2019, June 20). What is “medicare for all” and how would it work? NBCNews.com. https://www.nbcnews.com/politics/elections/what-medicare-all-how-would-it-work-n1014256
Sparks, G., Lopes, L., Montero, A., Presiado, M., & Hamel, L. (2026, April 30). Americans’ challenges with health care costs. KFF. https://www.kff.org/health-costs/americans-challenges-with-health-care-costs/
Sylvie, A. (2016, June 27). Single Payer Healthcare: Pluses, minuses, and what it means for you. Harvard Health. https://www.health.harvard.edu/blog/single-payer-healthcare-pluses-minuses-means-201606279835
Teirlinck, B., & Stoilova, D. (n.d.). Portable benefits: Unlocking innovation and job mobility | NYCEDC. NYCEDC. https://edc.nyc/research-insights/portable-benefits-unlocking-innovation-job-mobility
Telesford, I., Wagner, E., & Cox, C. (2025, October 6). How does the quality of the U.S. health system compare to other countries?. Peterson-KFF Health System Tracker. https://www.healthsystemtracker.org/chart-collection/quality-u-s-healthcare-system-compare-countries/#health-system-capacity
Thomas, K., & Regan, M. D. (2016, January 18). Sanders pitches tax hike to pay for Universal Health Care Plan. PBS. https://www.pbs.org/newshour/politics/sanders-pitches-tax-hike-to-pay-for-universal-health-care-plan
USAFacts Team. (2026, May 18). How many people in America skip medical treatment due to healthcare costs?. USAFacts. https://usafacts.org/articles/how-many-people-skip-medical-treatment-due-to-healthcare-costs/
World Bank Group. (2026). Life expectancy at birth, total (years) - United States, United Kingdom, Canada. World Bank Open Data. https://data.worldbank.org/indicator/SP.DYN.LE00.IN?end=2024&locations=US-GB-CA&start=2000
Enjoying my content?